Topic 2 Key concepts and Theoretical framework
Menopause is not a one-dimensional experience. It is biological, emotional, and social, shaped by both personal health and the environments where we live and work. For employers and employees alike, understanding menopause requires more than medical facts; it demands a holistic lens.
This section draws on two complementary models: the Biopsychosocial Model, which highlights the interaction of physical, psychological, and social factors, and the Health Belief Model, which explains how people assess risk, interpret symptoms, and decide whether to seek support. Together, they help us understand not only what women experience, but why responses to menopause can vary so widely.
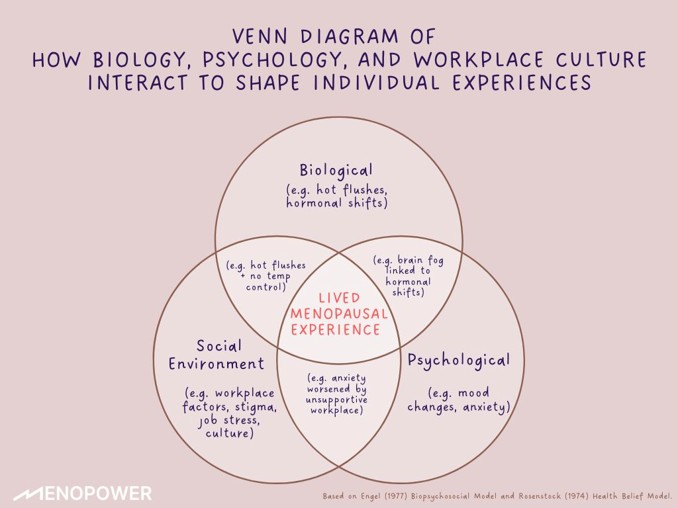
Understanding Menopause through the Biopsychosocial Model
The Biopsychosocial Model (Engel, 1977) views health not just as a physical condition, but as an outcome shaped by the interaction of biological, psychological, and social factors.
Applied to menopause, it helps explain why no two experiences are the same. Hormonal shifts (biological), emotional symptoms like anxiety or brain fog (psychological), and workplace culture, stigma, or lack of flexibility (social) all contribute to how menopause is experienced, and how well someone is supported.
Understanding this model allows us to move beyond symptom lists and address the full person: body, mind, and environment.
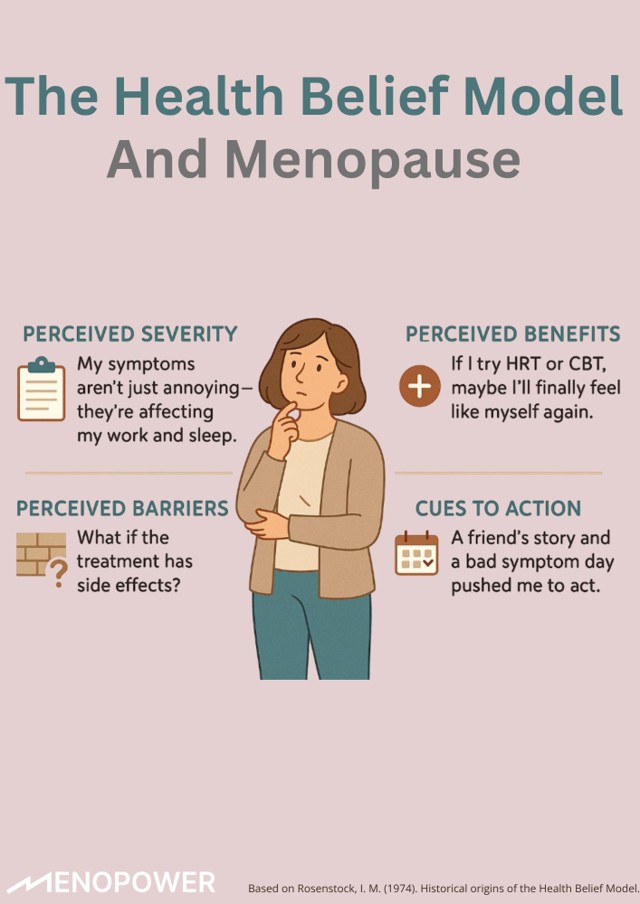
Understanding Decisions with the Health Belief Model
The Health Belief Model (Rosenstock, 1974) explains how people make decisions about their health. It focuses on what they believe about their symptoms, risks, and treatment options, not just what they know.
Applied to menopause, it helps explain why women respond so differently. Their choices around seeking support, using HRT, or even speaking to a doctor are shaped by four main things:
- Perceived severity of symptoms (how serious a woman thinks her symptoms are)
- Perceived benefits of taking action (what good things she expects from getting help)
- Perceived barriers such as things that get in the way (like fear, stigma or misinformation)
- Cues to action (triggers that prompt her to seek help, like a bad symptom day or advice from a friend)
Understanding these beliefs helps explain the real-life complexity of menopause decision-making, and why empathy and accessible information matter.
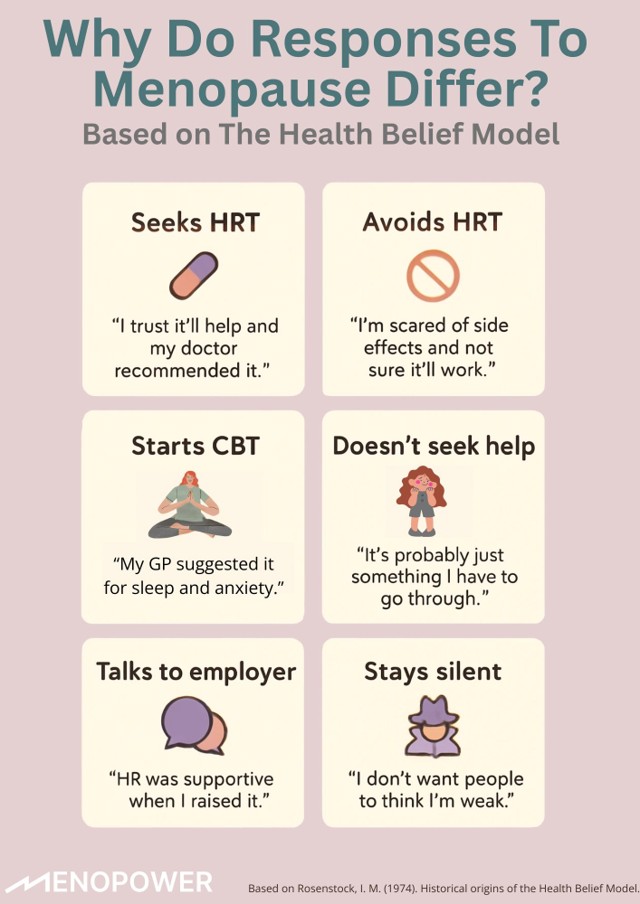
What This Means for the Workplace
- People with similar symptoms may respond very differently, based on beliefs about their symptoms, treatments, and how others will react, not just facts.
- Some avoid help due to fear, stigma, or past experiences. Others act after a single bad day or advice from a friend.
- Workplaces that offer empathy, clarity, and support remove key barriers to action.
- The goal isn’t to ‘convince’, it’s to create space for informed, empowered choices.
Treatment Options: HRT and Beyond
Hormone Replacement Therapy (HRT)
○What it is: Replaces oestrogen (± progesterone) to manage hormonal decline.
Benefits:
■Relieves hot flushes, joint pain, cognitive symptoms (“brain fog”), and sleep disruption
■May improve emotional stability and concentration
Types:
■Combined HRT (oestrogen + progesterone): for women with a uterus
■Oestrogen-only HRT: for women after hysterectomy
Risks:
■Slight increase in breast cancer risk (combined HRT, long-term use)
■Small risk of clots or stroke, especially with oral forms (lower with patches/gels)
Most benefits outweigh risks for women under 60 when monitored
Non-Hormonal Options
Psychological
■CBT (Cognitive Behavioural Therapy), mindfulness, and counselling, are scientifically supported options recommended to help manage menopausal symptoms
■Reduce anxiety, regulate sleep, improve mood
Medical:
■SSRIs/SNRIs (antidepressants), gabapentin
■May ease hot flushes and mood stability
Lifestyle & Complementary:
■Acupuncture, cooling techniques, nutrition, regular physical activity
■Often used by women who prefer non-hormonal or first-line interventions
Why This Matters
○Health Belief Model: Fear, confusion, or stigma can reduce treatment uptake
○Biopsychosocial Model: Menopause affects body, mind, and context; care must reflect this
○All women deserve clear information and access to personalised, evidence-based options
Download the ‘WOMEN’S HEALTH CONCERN FACT SHEET: HRT to learn more!
Download the ‘WOMEN’S HEALTH CONCERN FACT SHEET, HRT: Benefits and Risks to learn more!
Managing Long-Term Health Risks
The Challenge
As oestrogen declines during menopause, long-term health risks increase, including:
Musculoskeletal Syndrome of Menopause (MSM): joint pain, muscle loss, and stiffness

Osteoporosis: reduced bone density, higher fracture risk

Cardiovascular Disease (CVD): changes in cholesterol and heart risk
These risks are common but not inevitable, and often under-recognised.
Prevention and Protection
Hormone Replacement Therapy (HRT):
- Reduces osteoporosis risk by 28–50% depending on the type of fracture
- May also offer cardiovascular protection when started early (before age 60)
Lifestyle Factors:
- Regular weight-bearing and strength-building exercise
- Healthy nutrition (including calcium & vitamin D)
- Reduced alcohol, smoking cessation, stress management
Psychosocial Factors (Biopsychosocial Model):
- Sedentary work environments, low motivation, or mood issues can amplify risks
- Social support, encouragement, and education act as “enabling conditions”
Why This Matters
- Biopsychosocial Model: Health outcomes are shaped by physical habits, mental wellbeing, and social context
- Health Belief Model: Women who understand these risks and feel capable of addressing them are more likely to act
Cues to Action:
- Preventive screenings: Bone density scans (DEXA), cholesterol checks
- Health education at work or in clinical settings
- Normalising menopause-related musculoskeletal symptoms
Click here ‘British Heart Foundation: Menopause and your heart’ to learn more!
Download the ‘WOMEN’S HEALTH CONCERN FACT SHEET: Osteoporosis’ to learn more!
Download the ‘WOMEN’S HEALTH CONCERN FACT SHEET: Exercise in menopause’ to learn more!
Clarifying Medical Definitions
Why Definitions Matter
Understanding the stages and terms of menopause isn’t just academic, it shapes how women recognise symptoms, seek care, and make informed decisions. The Biopsychosocial Model reminds us that medical terms carry psychological and social weight, while the Health Belief Model shows that clear knowledge can prompt timely action.
Key Terms
Menopause: Permanent end of menstruation, confirmed after 12 consecutive months without a period. Usually occurs between 45–55 years, average age 51. May occur naturally or due to surgery/treatment.
Perimenopause: Transition phase before menopause. Hormone levels fluctuate, symptoms begin (e.g. irregular periods, hot flushes, mood changes). Typically begins in the mid-40s, but can start earlier.
Postmenopause: The phase after one year without periods. Hormone levels stabilise, but some symptoms (e.g. joint pain, hot flushes) may persist. Health risks (osteoporosis, CVD) increase.
Primary Ovarian Insufficiency (POI): Impaired ovarian function before age 40. Periods may become irregular or stop. Fertility can persist intermittently. Often caused by autoimmune/genetic factors or medical treatment. Requires HRT to prevent complications.
Premature Menopause: Permanent end of menstruation before age 40, due to natural causes, surgery, or treatment. Unlike POI, ovarian function does not return. Fertility is lost.
Download the European Menopause and Andropause Society’s (EMAS) ‘Menopause: definitions and terms’ factsheet to learn more!